Myth: I can see aspiration on an MBS but not with endoscopy.
Reality: Aspiration is clearly visible with endoscopy (right):
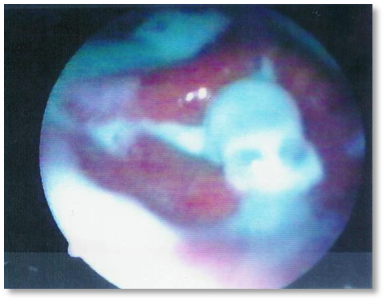
Reality: Aspiration is clearly visible with endoscopy (right):
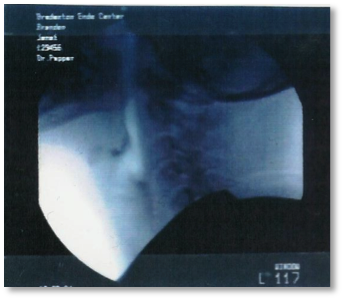
Myth: I can see everything I need to see on an MBS.
Reality: Secretions are invisible on MBS (left) but not with endoscopy (right):


Reality: Secretions are invisible on MBS (left) but not with endoscopy (right):
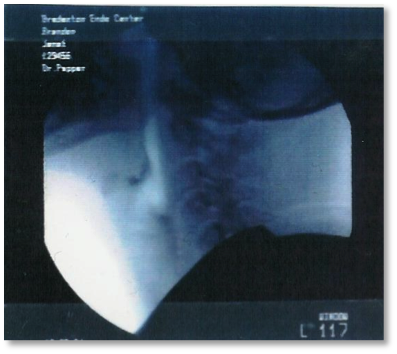
Myth: I need to see the esophageal stage of the swallow with the MBS to treat effectively.
Reality: Reflux or G-Tube feeding invisible on the MBS (left) and visible on endoscopy (right):

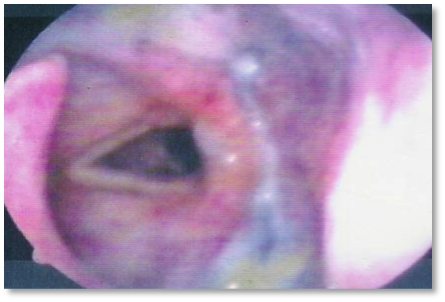
Reality: Reflux or G-Tube feeding invisible on the MBS (left) and visible on endoscopy (right):
Myth: I need to know the quantitative amount of aspirate for each aspirated consistency in order to treat effectively.
Reality: It is never just one consistency or one swallow, but rather a combination of issues that results in complications from dysphagia.
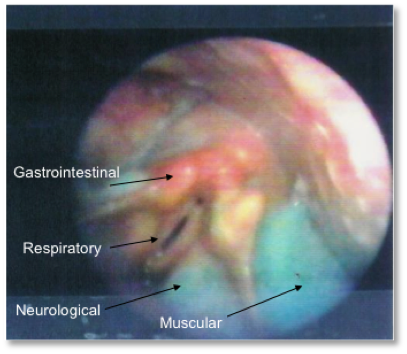
Reality: It is never just one consistency or one swallow, but rather a combination of issues that results in complications from dysphagia.